- Download PDF
-
- Executive Summary
- Introduction
- Rapid reconfiguration, rapid deployment, rapid results
- Why now?
- TRF tests are a subset of the diagnostics landscape
-
Five policy ideas for developing TRF test capacity
- Recommendation 1: U.S. research funding agencies should support the R&D and technological transition of TRF tests
- Recommendation 2: Congress should establish RADx as a permanently funded entity within NIH
- Recommendation 3: ASPR and CMS should foster sustainable demand for diagnostics through pre-purchase agreements and long-term reimbursement
- Recommendation 4: ASPR should prioritize an agile and reconfigurable Strategic National Stockpile model
- Recommendation 5: The FDA should streamline regulatory approval to evaluate TRF tests based on their benefits for public health
- We can have better tests, if we want them
Executive Summary
Diagnostic testing plays a crucial role in managing infectious disease outbreaks. But the ideal diagnostic strategy is not one-size-fits-all. The relative importance of test attributes such as development speed, affordability, and accessibility depends on the specific use case and the characteristics of the outbreak. Consequently, different frameworks have emerged to guide diagnostic strategies across different contexts. The World Health Organization’s (RE)ASSURED criteria, for instance, define the ideal diagnostic test for resource-limited settings. Additionally, epidemiologists have outlined key principles for public health testing, where the focus shifts from individual diagnosis to improving population health.
While these frameworks provide valuable guidance, they do not specifically address one particularly important scenario: outbreak control. The COVID-19 pandemic exposed significant weaknesses in global diagnostic capabilities, with most countries flying blind through the critical early days of the pandemic. Without widespread testing, public health systems relied on broad interventions like lockdowns and travel restrictions. Other recent outbreaks, like the 2024 mpox surge and H5N1 bird flu, highlight our persistent inability to rapidly scale up testing for emerging and novel pathogens.
We believe it’s time for a conceptual shift in our approach to outbreak diagnostics. Instead of accepting months-long development timelines as inevitable, we should aim to deploy tests within days of detecting an outbreak. Widespread rapid testing could help transform our public health strategy from reactive and sweeping to proactive and precise.
Here, we introduce a Triple Rapid Framework (TRF) for outbreak control, aiming to deploy 10,000 point-of-person tests within ten days of outbreak detection, each providing results in one minute. In the early stages of an outbreak, these tests could be rapidly distributed to high-risk areas, allowing for immediate identification and isolation of cases and potentially preventing widespread transmission.
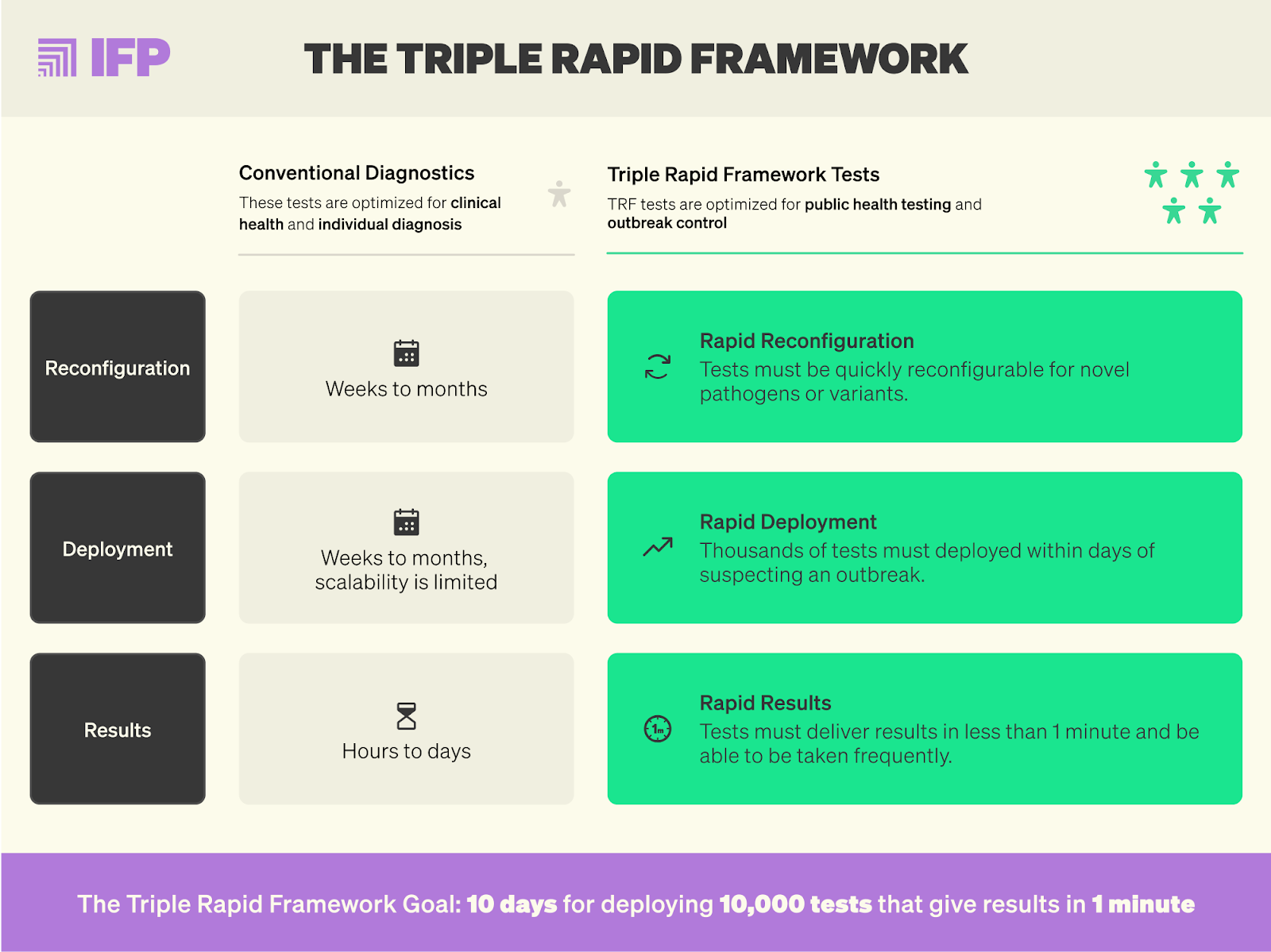
The Triple Rapid Framework builds on existing frameworks like REASSURED, but prioritizes three essential features for effective outbreak control:
- Rapid reconfiguration: Tests must be designed for quick adaptation in response to novel pathogens or variants, with updates possible within hours.
- Rapid deployment: Tests should be point-of-person tests with simplified supply chains, allowing for straightforward distribution across diverse settings.
- Rapid results: Tests should give results within less than a minute, ensuring immediate action can be taken.
Since 2020, strategic U.S. government investments have helped shift the diagnostics paradigm from lab-based tests to free COVID-19 tests delivered to doorsteps. Even better testing solutions, including for novel pathogens, are on the horizon. But even though rapid tests are a U.S. biodefense priority, the companies producing them face a deadly combination of regulatory uncertainty and lack of demand. What’s more, no coordinating national plan for diagnostics exists.
A shift towards the Triple Rapid Framework demands innovation and coordination across the entire diagnostic pipeline, from research and development to regulatory approval and manufacturing. To realize this ambitious vision, we propose a coordinated effort involving multiple U.S. government agencies working in close partnership with the private sector:
- Research funding agencies like the NIH, BARDA, ARPA-H, and DARPA should support the R&D and technological transition of a broad portfolio of innovative testing technologies, such as instrument-free rapid PCR, at-home isothermal amplification tests, multiplexed CRISPR-based tests, and improved antigen tests.
- Congress should establish RADx as a permanently funded entity within the NIH to ensure ongoing support for diagnostic innovation, validation, and approval.
- ASPR and CMS should foster sustainable demand through pre-purchase agreements and long-term reimbursement strategies, ensuring that diagnostic innovation remains economically viable.
- ASPR should prioritize an agile and reconfigurable Strategic National Stockpile model to ensure rapid availability of testing resources during emergencies, regardless of the pathogen in question.
- FDA should streamline regulatory approval processes for public health screening tests and simplify the process for incorporating new pathogens into existing diagnostic platform technologies.
Introduction
During emerging infectious disease outbreaks, the time to most effectively prevent a pathogen from spreading is at the outset, when we often know the least. The delayed development and approval of COVID-19 tests had societies worldwide flying blind through the early months of the pandemic. For instance, scientists estimate that by March 2020, testing in the U.S. had identified less than 1% of all SARS-CoV-2 infections. In the absence of accessible testing, many public health systems enacted broad and sometimes draconian interventions such as travel restrictions, lockdowns, and quarantines, with substantial health, economic, and societal costs.
In an era of precision cancer treatments and gene therapies, we should not have to impose widespread quarantines on individuals with unknown infection status. We can and should do better. Just like mRNA vaccines revolutionized vaccine development, we now have wonderful diagnostic tools to detect infections non-invasively and at scale. During the COVID-19 pandemic, some nations, like South Korea, swiftly implemented widespread testing and contact tracing, flattening the epidemic curve at a manageable social cost.
Other countries, including the U.S., struggled to achieve similar outcomes. The Centers for Disease Control and Prevention (CDC) initially set strict guidelines for COVID-19 polymerase chain reaction (PCR) testing due to test shortages. The first U.S. patient hospitalized with COVID-19 of unknown origin (possibly indicating community transmission) initially failed to meet the CDC’s testing criteria, leading to a four-day diagnostic delay. PCR test kits produced by the CDC had a basic design flaw and were likely contaminated; and it wasn’t until February 29th, 2020, that the Food and Drug Administration (FDA) relaxed its rules around using tests from academic laboratories and private companies.
Consequently, by March 17th, 2020, the U.S. had tested around 400 people per million for COVID-19. South Korea, in contrast, had tested more than 5,000 people per million.
The lack of testing significantly hindered early containment efforts in the U.S., contributing to the spread of the virus. Modelling research estimates that a hypothetical nationwide antigen testing strategy, running from June to December 2020, could have saved more than 100,000 lives and increased GDP by at least $395 billion. Delays in accessible, widespread testing have similarly hindered responses to other recent outbreaks, including the 2022 and 2024 mpox outbreaks and the 2024 H5N1 bird flu outbreak in U.S. cattle.
Currently, most countries are too slow in developing, approving, and manufacturing diagnostics to be able to control infectious disease outbreaks at their source — particularly those caused by variants or novel pathogens with pandemic potential. But fast, frequent, and scalable testing solutions, including for novel pathogens, are on the horizon. Compared to 2019, the U.S. government has made great strides to make cheap and accurate tests available to the masses. The Rapid Acceleration of Diagnostics (RADx) program and the Department of Health and Human Services’ (HHS) Testing and Diagnostics Working Group led strategic investments in at-home tests and domestic manufacturing. Between January and March 2022, the Postal Service delivered free COVID-19 tests to more than half of U.S. households.
Nonetheless, it took eight months for the first COVID-19 over-the-counter (OTC) rapid test to receive Emergency Use Authorization (EUA) from the FDA. This timeline falls short of the 2022 U.S. National Biodefense Strategy’s goal to develop rapid point-of-need tests within 90 days of identifying a biological incident. The Biomedical Advanced Research and Development Authority (BARDA) has set itself a more ambitious goal: to deploy more than 100 million pathogen-specific tests within 45 days of a public health emergency declaration.
While this goal is laudable, we should be more ambitious still. 45 days after COVID-19 was declared a Public Health Emergency of International Concern, New York City shut down its public school system, and state health departments circulated guidelines for who would receive ventilator care in the event of shortages.
To fully reap the public health benefits of rapid tests, we should aim not only to match the pace of evolving pathogens, but to stay several steps ahead. To transform tests into useful tools for outbreak control, rather than eventual outbreak triage and management, we need to reconfigure and deploy rapid tests within days of detecting an outbreak.
We propose a “Triple Rapid Framework” (TRF) for specialized pandemic prevention tests, prioritizing rapid reconfiguration, rapid and scalable deployment, and rapid results. The TRF goal is to deploy 10,000 at-home tests within 10 days that give results within 1 minute. We acknowledge that this is an ambitious goal. However, based on an extensive literature review and interviews with more than 20 experts across government, the private sector, nonprofits, and academia, we believe that with appropriate resources and attention, this goal is well within reach.
In the early stages of an outbreak, TRF tests could be rapidly distributed to high-risk areas, allowing for immediate identification and isolation of cases and potentially preventing widespread transmission. TRF testing could help transform our public health strategy from reactive and generalized to proactive, precise, and effective.
Rapid reconfiguration, rapid deployment, rapid results
Different frameworks for diagnostic testing exist. The World Health Organization’s (RE)ASSURED criteria, for instance, define the ideal diagnostic test for resource-limited settings. Others have outlined key principles for public health testing, where the focus shifts from individual diagnosis to improving population health. While these principles provide valuable guidance, they are not specifically focused on outbreak control. TRF tests, in contrast, prioritize three essential features for effective outbreak control and pandemic prevention:
- Rapid reconfiguration: The dynamic nature of pathogens demands a testing approach that is equally adaptable. Tests must be designed for quick reconfiguration in response to novel pathogens or variants. Test developers should strive to create platforms where updates can be made in a few days without overhauling the entire system; and regulatory approaches should enable swift approval of these updated tests.
- Rapid deployment: In an outbreak scenario, the scalable distribution and decentralized implementation of tests become as important as their accuracy. TRF tests will be point-of-person tests with simplified supply chains, permitting straightforward deployment across diverse settings, including resource-limited settings. At-home testing allows individuals to make risk-based decisions from the privacy of their homes and reduces inequalities in testing access. Furthermore, OTC rapid tests can link diagnosis to timely treatment where available. They also enable repeated testing, which is crucial for healthcare personnel with repeated exposures, pathogens with several-day incubation times, or pathogens that transmit in the absence of symptoms.
- Rapid results: Tests must have a short result turnaround time, ideally under one minute, to ensure that immediate action can be taken. For screening tests to be widely adopted by the public during the critical early stages of an outbreak, they must be as accessible and low-friction as possible. For example, rapid results are critical for efficient entry screening and contact tracing, where a wait of 15 minutes versus one can make the difference between whether screening is implemented or not. A 15-minute wait time requires in-advance planning, space for people to wait, and potentially discourages implementation altogether. In contrast, a test that delivers results within one minute makes widespread adoption much more feasible.
TRF tests could also play a crucial role in managing endemic diseases such as influenza or Respiratory Syncytial Virus (RSV) infection. Respiratory disease corresponds to an estimated cost of more than $100 billion dollars annually in lost work and medical costs in the U.S. alone. Widespread testing could inform self-isolation and treatment and reduce the high burden of respiratory disease in regular sick seasons. Reconfiguration could be done seasonally, ensuring that tests are optimally effective against different variants and subtypes.
Why now?
A recurring theme emerged from our expert interviews was that the U.S. is at risk of squandering the critical lessons learned from COVID-19 testing. As the urgency of the pandemic has waned, so has government support for diagnostics. Many innovative companies that received U.S. taxpayer money during the pandemic now face a deadly combination of demand and regulatory uncertainty.
Consider the example of Lucira: In February 2023, the FDA approved the first OTC test for COVID-19 and the flu, created by Lucira — on the very day Lucira filed for bankruptcy, citing the prolonged FDA approval process as a contributing factor.
Furthermore, while the CDC has launched promising initiatives like its Traveler-based Genomic Surveillance program and the National Wastewater Surveillance System, gaps in U.S. biosurveillance persist. H5N1 has infected 442 cattle herds in 14 states, and 44 human cases have been reported. Yet by November, no rapid at-home tests specifically detecting H5N1 were available.
Further complicating matters, the FDA recently moved to tighten regulations on laboratory-developed tests (LDTs), While the FDA’s intention to ensure test quality through rigorous reviews is commendable, hospital and public health labs caution that this stringent approach could slow diagnostic test development in public health emergencies.
During the COVID-19 pandemic, we witnessed firsthand how bureaucratic red tape can impede the availability of tests. Traditionally, clinical laboratories have developed and run their own tests without FDA oversight. Instead, laboratory testing is regulated by the Centers for Medicare & Medicaid Services (CMS) through the Clinical Laboratory Improvement Amendments (CLIA). However, in early 2020, the FDA suggested that EUA is needed for SARS-CoV-2 LDTs, creating a bottleneck precisely when testing expansion was crucial. Moving forward, regulatory and public health agencies must carefully calibrate oversight to ensure safety without stifling the agility needed in public health crises.
TRF tests are a subset of the diagnostics landscape
An ideal biosurveillance system incorporates multiple layers, including:
- Individual clinical testing for symptomatic patients to inform patient care.
- Public health screening for asymptomatic individuals in settings like hospitals, schools, or nursing homes.
- Surveillance testing to track the spread of a pathogen.
Beyond these layers, a comprehensive biosurveillance system must also deploy a variety of diagnostic tools across diverse environments. These tools include:
- Lab-based diagnostics like PCR tests conducted in centralized laboratories.
- Point-of-care testing performed at the time and place of patient care.
- Point-of-person testing for individual use at home or in resource-limited settings.
At-home delivery and rapid results are essential features that set TRF tests apart from lab-based tests such as PCR, which often take several hours to deliver results. However, lab-based tests can still complement TRF tests, especially in the early stages of an outbreak. During the COVID-19 pandemic, South Korea quickly set up hundreds of high-capacity PCR screening facilities, allowing the country to test early and frequently. As suggested by the Testing Playbook for Biological Emergencies, the first FDA-authorized pathogen-specific test should be deployed to the U.S. Laboratory Response Network and Public Health Laboratories within 48 hours after determining a potential biological incident. This would allow lab-based PCR tests to act as a vital interim measure until TRF tests are widely available for at-home delivery.
Another characteristic of infectious disease diagnostics is whether they detect one or several targets. Targeted tests are designed to identify a single specific pathogen, whereas multiplexed tests can detect multiple pathogens at once. This is particularly valuable for respiratory or gastrointestinal illnesses, where multiple pathogens may present with similar symptoms. A third category is pathogen-agnostic tests, designed to detect a wide range of pathogens, including unknown ones. Pathogen-agnostic tests are often based on metagenomic sequencing technologies, which analyze the entire genetic content of a given sample.
Targeted and multiplexed tests, rather than pathogen-agnostic tests, will likely be best suited to achieve the desired TRF combination of rapid reconfiguration, rapid and scalable deployment, and rapid results. Pathogen-agnostic tests are not in routine clinical use due to high costs and complex workflows. While government programs invest in agnostic diagnostics and experts have outlined a roadmap for a low-cost, rapid pathogen-agnostic metagenomic sequencing device, a device meeting these criteria is projected to be at least several years away. Furthermore, during an emerging outbreak, the focus typically narrows to identifying one specific pathogen, making targeted or multiplexed tests particularly valuable.1
Five policy ideas for developing TRF test capacity
TRF tests require sustained government R&D support, streamlined regulatory approval, and a clear path to market to come to fruition. Although our policy recommendations are tailored to the U.S., the benefits of rapidly deployable TRF tests will be global. Given sufficient government and philanthropic funding, TRF tests could help provide equitable access to diagnostics and empower low- and middle-income countries to respond effectively to emerging health threats.
Drawing from our expert consultations, we propose a coordinated policy strategy involving regulatory agencies, public health bodies, and governmental and philanthropic funders to achieve the goal of TRF tests within the next two to five years.
Recommendation 1: U.S. research funding agencies should support the R&D and technological transition of TRF tests
Governments and philanthropic funders should aim to invest in a broad R&D portfolio to achieve TRF tests. It is premature to narrow our focus to a single detection method or sampling type. Potential technology solutions span detection methods such as antigen tests, nucleic-acid amplification tests (NAAT), and array-based tests, as well as different sample types such as saliva, blood, or breath.
The 2022 U.S. National Biodefense Strategy and Implementation Plan proposes a diagnostics joint capabilities plan (Goal 3.2) across several federal agencies. The National Institutes of Health (NIH), BARDA and its Division of Research, Innovation, and Ventures (DRIVe), the new Advanced Research Projects Agency for Health (ARPA-H), and the Department of Defense with its Chemical and Biological Defense Program and the Defense Advanced Research Projects Agency (DARPA) are particularly well-positioned to advance TRF test R&D. For example, Objective 1.1 of BARDA’s Strategic Plan proposes to invest in tests that “can be rapidly adapted to emerging threats” and “move testing closer to the patient.”
NAAT tests offer advantages over current antigen tests, including lower limits of detection and faster reconfiguration. Recent advances in NAAT point-of-care test technology include instrument-free, rapid PCR tests and isothermal nucleic acid amplification tests. Another testing approach is array-based tests, like those based on the CRISPR technology. CRISPR-based tests can be massively multiplexed, detecting hundreds or even thousands of pathogens simultaneously.

While at-home NAAT and CRISPR-based tests show promise, they are not in widespread use today. Next to the continued need to advance R&D, a key challenge lies in driving down production costs to make these tests competitive with traditional antigen tests. To unlock the full potential of these advanced diagnostics, targeted government support for R&D and long-term reimbursement will be crucial.
Antigen tests, with their proven track record, will likely remain an important part of our at-home testing portfolio. However, developing antigen tests currently takes weeks to months and often involves immunizing animals, such as rabbits, with the target antigen to produce the corresponding antibodies. By finding ways to rapidly identify and scale antibodies or by creating libraries of relevant broad-spectrum antibodies for pathogens of concern prior to the next outbreak, test development could be significantly accelerated.
In addition, lateral flow antigen tests could be further optimized to improve sensitivity and specificity without sacrificing speed or affordability. Investments in molecules like aptamers and oligomeric peptides should be continued to manufacture synthetic antibodies that are more robust and quicker to manufacture than traditional antibodies. These molecules could be incorporated into lateral flow assays or sensor-coupled tests like breath tests to detect pathogens with high sensitivity and specificity.
Recommendation 2: Congress should establish RADx as a permanently funded entity within NIH
While U.S. government agencies like the NIH and BARDA have long backed R&D for diagnostics, a specialized HHS program was absent until the NIH launched its Rapid Acceleration of Diagnostics (RADx) program for COVID-19 diagnostics. RADx contributed to a substantial increase in testing capacity, with RADx-backed companies supplying more than 6.7 billion tests to the U.S. market from late 2020 through Q4 of 2022.
RADx rapidly de-risks and validates tests and supports diagnostic companies through the intricate process of optimizing test performance and obtaining FDA approval. For example, RADx’s Independent Test Assessment Program (ITAP) collaboration with the FDA has accelerated the regulatory review of diagnostics, including for OTC and multiplexed tests.
RADx’s value also arises from integrating tests into personal and public health programs, ensuring their application across diverse settings. Together with programs like the CDC’s Increasing Community Access to Testing (ICATT) program, RADx’s focus on accessible design principles and its RADx-UP program for underserved populations ensured tests were moved into communities quickly. To sustain RADx’s success, it should be established as a permanent initiative within NIH to support test R&D and regulatory approval for infectious disease diagnostics.
Recommendation 3: ASPR and CMS should foster sustainable demand for diagnostics through pre-purchase agreements and long-term reimbursement
During the COVID-19 response, the U.S. government established critical partnerships with private-sector test manufacturers and commercial clinical laboratories that helped scale up testing capacity nationwide. However, these demand signals came late and were often implemented only as short-term measures. To rapidly ramp up testing capacity in future crises, the U.S. government needs to work more closely with the private sector in non-pandemic times.
Public health experts have proposed a National Diagnostics Action Plan that suggests establishing pre-event and routine contracts to reduce market uncertainty for the private sector. For example, the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR) could invest in standing capabilities within commercial and academic labs through pre-purchase agreements, preserving critical expertise and infrastructure in non-pandemic times.
Furthermore, CMS should develop a mechanism to expedite reimbursement for tests targeting emerging pathogens, as well as increase their payment rates. During the COVID-19 pandemic, CMS increased its rates for lab-based testing, which was crucial in incentivizing the expansion of lab-based testing capacity. To encourage the development of multiplexed diagnostics, CMS should offer higher compensation — for example, a payment increase of 1.5 times the standard rate for pathogen-specific tests.
Philanthropic foundations and global health nonprofits could contribute by funding and coordinating the procurement of TRF tests for resource-limited settings. For example, by funding global health nonprofits like the Foundation for Innovative New Diagnostics (FIND), the Gates Foundation has been instrumental in developing and validating rapid tests for the developing world.
Recommendation 4: ASPR should prioritize an agile and reconfigurable Strategic National Stockpile model
Supply chain bottlenecks significantly limited the availability of COVID-19 tests during the early stages of the pandemic. However, as Ryan Remmel previously pointed out, governments cannot stockpile pathogen-specific tests for future pandemics without prior knowledge of the pathogen in question. An agile Strategic National Stockpile (SNS) model would keep a warm manufacturing base and enhance readiness among industry partners.
Currently, the SNS manages most of its inventory itself, and replacing expiring supplies comes with a significant cost. To address this, the SNS has developed a Vendor-Managed Inventory (VMI) system, enabling manufacturers to hold supplies on-site and regularly rotate stock to replace expiring items. This VMI system could be expanded.
Stockpiled materials in the SNS should include basic components like nitrocellulose used in lateral flow tests or swabs, which were a critical bottleneck during the COVID-19 response. ASPR’s new Office of Industrial Base Management and Supply Chain could oversee this initiative, coordinating with various partners across the federal government and private industry.2
Additionally, recent advances in modular and automated manufacturing of NAAT-based tests and next-generation CRISPR diagnostics have made it possible to quickly adapt test kits to emerging pathogens. The SNS should move towards a reconfigurable stockpile model, where it stores not only test components but also reconfigurable test kits that can be quickly reconfigured due to their modular design.
Recommendation 5: The FDA should streamline regulatory approval to evaluate TRF tests based on their benefits for public health
In June 2020, the CDC estimated that the actual number of COVID-19 cases in the U.S. was ten times higher than the number of test-confirmed cases. Despite the high sensitivity of PCR tests, these tests could detect, at best, 10% of all infections due to their limited accessibility. Then-CDC director Rochelle Walensky stated in September 2020 that for screening to prevent SARS-CoV-2 outbreaks, “saliva-based antigen is better than the PCR swab.”
Nonetheless, the FDA authorized the first at-home rapid test only on November 17th, 2020 — eight months into the pandemic, at a time when countries like Slovakia and the United Kingdom successfully performed mass testing with rapid tests. Starting in October 2020, Slovakia tested large parts of its population of 5.5 million with rapid antigen tests and found more than 50,000 positive cases. After two rounds of testing and isolation and quarantine of household members of those testing positive, infection prevalence decreased by about 80%.
Countries like Slovakia understood that repeated COVID-19 rapid antigen testing of asymptomatic and symptomatic patients can achieve performance comparable to PCR tests, demonstrating the practical value of considering test accuracy within the larger context of public health needs. Unlike PCR tests, which often require specialized labs and longer processing times, rapid tests offer swift results and allow for repeated self-testing, making them valuable public health tools for detecting infectiousness on a large scale.
However, the FDA lacks a specific regulatory framework for public health screening tests. OTC tests are subject to the same stringent standards for clinical trial data and analytic accuracy as those applied to diagnostics for individual clinical health. During the COVID-19 pandemic, this one-size-fits-all approach resulted in some of the FDA’s requirements becoming practically unattainable for OTC tests, delaying the authorization of rapid tests and substantially restricting their availability in the U.S.
To be better prepared for the next outbreak, the FDA should adapt its regulatory frameworks to ensure public health tests are evaluated based on criteria that align with their intended use and benefits for society:
- The FDA should issue an internal guidance document that outlines how to weigh public health benefits for infectious disease diagnostics, considering favorable attributes like rapid results, accessibility, and scalability against the risks of false positives or negatives. Such tests would be evaluated differently from those used for individual medical diagnosis, recognizing their distinct role in public health emergencies. Alternatively, Congress could direct the FDA to introduce a new authorization pathway for evaluating and approving public health surveillance and screening tools.
- In May 2024, the FDA released an updated draft guidance for a Platform Technology Designation Program to simplify the regulatory process for new drugs based on the same platform technology. Similarly, the FDA should simplify the process for incorporating new pathogens into OTC testing platforms. COVID-19 catalyzed the development of the first at-home NAAT tests, which can be adapted to other pathogens more easily than traditional antigen tests. Other innovative testing platforms that can be reconfigured within days are on the horizon.
- To better balance the burden of proof required for EUA, tests that demonstrate efficacy through pre-clinical data should be approved initially, followed by rigorous real-time performance monitoring. Should subsequent real-world data or clinical trials identify more accurate alternatives, the FDA can revoke the EUA of any test that underperforms, ensuring that only the most effective tools remain in use.
- At-home testing offers a privacy-preserving solution that sidesteps the political tensions associated with vaccines and mask mandates. However, public perception of diagnostics often fixates on accuracy alone. For public health testing, it’s crucial to shift this mindset through targeted education campaigns, highlighting the importance of multiple factors like speed, testing frequency, accessibility, and yes, accuracy — but as part of a broader picture. The FDA should play a crucial role in educating the public, communicating that public health testing is not just about individual results — it’s about keeping our loved ones and communities safe.
We can have better tests, if we want them
The economics of prevention present a compelling case for investing in specialized outbreak control tests. By allocating resources to develop these tools proactively, we can potentially avert the astronomical economic and societal costs associated with outbreaks spiraling out of control into epidemics and pandemics.
Triple Rapid Framework tests, characterized by their rapid reconfiguration, rapid deployment, and rapid results, could represent a paradigm shift in infectious disease testing. The question now is not whether we can have better tests, but whether we have the collective will to make them a reality.
We thank Jassi Pannu, Arielle D’Souza, Michael Mina, and Kevin Land for their valuable contributions to this piece. We also thank Chris Achar, Emmanuel Agogo, Janice Chen, Elliot Cowan, Jeffrey Gibbs, Mark McClellan, Cameron Myhrvold, Roarke O’Brien, Christian Schafmeister, Bruce Tromberg, and additional anonymous experts from government, academia, industry, and the nonprofit sector for their willingness to participate in expert interviews. The conclusions in this piece do not necessarily imply endorsement or unanimous consensus by the interviewees and their organizations.
-
For instance, nucleic-acid-based amplification tests can be rapidly reconfigured for a new pathogen based on nucleic acid sequence data. In contrast, antigen test development often takes longer, as the design of the corresponding antibodies used in a test may take weeks to months.
-
Next to ASPR in the U.S., agencies worldwide can be explicitly tasked with stockpiling, such as the Health Emergency Preparedness and Response Authority (HERA) in the European Union or Africa CDC.