On August 10th, the Institute for Progress filed the following comment in response to BARDA’s Request For Information on ways Project NextGen could ensure future COVID-19 vaccine technologies bolster preparedness against future variants.
Introduction
The $5 billion Project NextGen announced earlier this year represents a pivotal step forward in the ongoing battle against infectious disease. It advances SARS-CoV-2 vaccine candidates that induce broader and more durable immunity, while exploring new delivery methods, like intranasal vaccination, that may increase transmission-blocking.
Operation Warp Speed set a new standard for what is possible in terms of speed and scope, and is thus a model for what the best version of Project NextGen can look like. The recent $500 million given in awards are indicative of Project NextGen’s rapid progression.
We recently examined the existing Target Product Profile (TPP) criteria for Project NextGen, and believe that focusing on attributes that can foster broader protection and reduce viral transmission in particular will help ensure Project NextGen is a success.
Target Product Profiles
Q1: Are there additional vaccine characteristics missing, or are there any currently on the list you would remove and why?
- Pan-Betacoronavirus Protection Optimal Attribute: We recommend the inclusion of an optimal attribute for pan-betacoronavirus protection. The betacoronavirus genus includes not only SARS-CoV-2, but also the MERS-CoV virus and two common cold coronaviruses (OC43 and HKU1). Conferring cross-protection against these viruses would be valuable not only for COVID-19, but also for other circulating and novel human-infecting betacoronaviruses. One well-supported forecast for the expected value of a betacoronavirus vaccine authorized before 2028 is a median of 55.5k deaths averted in the U.S. from 2028-2030 alone.
- Viral Transmission Reduction Threshold Attribute: A vaccine’s potential to reduce onward viral transmission should be considered as a threshold attribute. There is currently an optimal attribute target, but no threshold target: ~50% reduction in transmission could be set as a threshold level. In the event of another Omicron-type event, where a new SARS-CoV-2 variant arises that is as different from current-circulating Omicron subvariants as Omicron BA.1/BA.2 was from Delta, this level would substantially dampen overall transmission.
Q2: Are there any target performance levels that should be modified and why?
While other vaccine characteristic requirements are important, most of them should be de-emphasized. Their target performance levels should be secondary to targets relating to the breadth of protection (1a) and viral transmission reduction (1b) for reasons explained in 4a and 4b. In particular, formulation stability requirements should be modified to be less stringent.
- Formulation stability requirements: There is a “Shelf life stability & Storage” threshold of the finished product being stable for >1 year at 2-8°C, and an optimal target of >2 years at 2-8°C. However, many consumer freezers can achieve temperatures as low as -18°C, low enough for vaccine storage. To take one example, the Moderna mRNA vaccine can be stored between -50°C and -15°C until expiration, which means that even higher-grade consumer freezers are well capable of storing vaccines. Moreover, the Moderna mRNA vaccine can be stored at temperatures between 2°C and 8°C for up to 30 days, within the range of temperatures achieved by normal refrigerators. Thus, formulation stability should not be seen as a major concern for the U.S., although it can be for low-and-middle-income countries (LMICs). Fortunately, in LMICs, many initiatives launched during the COVID pandemic have improved the cold chain capacity and vaccine delivery — for example, UNICEF procured about $165 million worth of cold chain equipment and services in 2022 alone.
Q4: Which of these product attributes are most important to our health security preparedness and why?
- Broadly Neutralizing Protection: Broadly neutralizing protection against coronaviruses is crucial for global health security preparedness. The coronavirus family has been the source of several epidemic and pandemic threats in recent history, such as SARS, MERS, and COVID-19. Pan-betacoronavirus or even pan-coronavirus protection would provide a robust defense against these known threats, as well as potential future emergences of novel coronaviruses.
- Transmission Blocking: In addition to preventing illness in the vaccinated individual, the ability to block transmission is vital for controlling the community spread of the disease. Traditional vaccine development has often focused on individual protection, leaving community-level transmission reduction as a secondary consideration. However, vaccines that can break the chain of transmission slow the emergence of new variants and protect those who cannot be vaccinated. Unfortunately, there is a clear market failure in this area, as vaccine recipients generally do not bear the cost of community transmission. This misalignment of incentives can lead to underinvestment in vaccines that block transmission. Public policy and funding must address this market failure to ensure that vaccines are not only effective in individual protection but also in reducing the risk of widespread transmission.
Q5: Which of these product attributes would most incentivize end users (patients, caregivers, clinicians) to choose to get vaccinated?
- Ability to Reduce Transmission: A significant driver for public uptake would be the demonstrated ability of a vaccine to reduce transmission. The assurance that getting vaccinated not only protects the individual but also prevents them from infecting loved ones can motivate people to get vaccinated.
- Mucosal Route of Administration: A non-needle mucosal route of administration can increase vaccine uptake, especially among those with needle phobia. More importantly, an intranasal, oral or skin patch route of administration would likely be more effective overall, since these target the mucosa — and mucosal vaccines are thought to be substantially more likely to reduce transmission.
- Minimal Dose Administration: Minimal dose administration — a single dose, or a primary dose with one booster — will be more appealing to the public, due to convenience. This could quickly improve population-level immunity by increasing the number of people who can be vaccinated at the early stages of vaccine rollout.
Q7: Are there any other features of the TPP that may improve availability in low-middle income country settings, expanding the global reach of vaccines that may be eligible for prizes?
- Mucosal Route of Administration: Vaccines that can be administered orally, intranasally, or via skin patch would also be beneficial. These routes of administration do not require trained healthcare professionals, and could potentially be self-administered. This would significantly improve accessibility in areas with limited healthcare resources, and improve the feasibility of widespread vaccination in a global catastrophic biological event.
Measuring a product’s ability to meet the objective
Q1. How should product developers prove that their vaccine meets or exceeds the TPP attributes?
Product developers should employ a comprehensive approach involving in vitro assays, animal models, and human clinical trials to demonstrate that their vaccine meets the TPP attributes.
- In vitro assays: Developers should leverage in vitro assays to evaluate the impact of their vaccines on the virus life cycle. For instance, in studies of malaria, potential inhibitors were evaluated on their ability to block the development of the Plasmodium’s sexual stages crucial for transmission from humans to mosquitoes. Similarly, for SARS-CoV-2, assays could be designed to evaluate how vaccine-induced immune responses can interfere with viral replication, neutralize the virus, and thus prevent its transmission. BARDA or a consortium of companies could help develop standardized assays for measuring mucosal immunity, which is particularly relevant for intranasal vaccines. These could include assays to measure the levels of IgA antibodies in samples taken from the mucosal surfaces.
- Animal models: Animal models can provide insights into infection dynamics and transmission potential of SARS-CoV-2, and help evaluate the efficacy of potential vaccines. For instance, a SARS-CoV-2 study demonstrated that the orally administered antiviral MK-4482/EIDD-2801 significantly reduced SARS-CoV-2 load in the upper respiratory tract of ferrets and suppressed spread to untreated contact animals, indicating its potential for blocking transmission.
- Human challenge trials: Human challenge trials involve intentionally infecting vaccinated volunteers with the virus. While this approach is ethically sensitive and requires careful consideration of risks, it can provide direct, robust evidence of a vaccine’s ability to prevent infection and transmission. Challenge trials allow for precise control of variables, such as the viral strain used for infection and the timing of infection post-vaccination. Furthermore, human challenge trials can be conducted with a relatively small number of participants, making them more feasible and efficient compared to large-scale field trials.
- Real-world studies: Observational studies in real-world settings are crucial to evaluate the impact of a vaccine on transmission. Household transmission studies, like the SARS-CoV-2 transmission study recently done in the UK, can provide insights into the dynamics of viral spread without necessitating tens of thousands of participants. In these studies, researchers can assess infection rates in vaccinated and unvaccinated individuals within households and use genomic sequencing data to track the spread of specific virus strains.
3. What trials, assays, tests, processes, etc. will need to be developed to be able to prove a product can meet or exceed optimal product attributes?
Several new tools and methodologies will need to be developed to accurately evaluate a vaccine’s product attributes:
- Assays for mucosal immunity: Given that SARS-CoV-2 is primarily transmitted through aerosols generated in the upper respiratory tract, it is crucial to develop better assays for measuring immunity in these areas. These could include both in vitro methods such as ELISA for measuring antibody levels at mucosal surfaces (like nasal swabs for intranasal vaccines), and in vivo methods involving animal models to study local immune response at mucosal surfaces.
- Cross-neutralizing Antibody Assays: To evaluate the breadth of protection offered by pan-coronavirus vaccines, assays that can measure the ability of vaccine-induced antibodies to neutralize various coronaviruses are needed.
- Next-Generation Technologies: Advanced technologies such as single-cell RNA sequencing can provide a detailed understanding of the immune response to vaccination. In addition, next-generation sequencing technologies can track viral evolution in vaccinated individuals — providing insights into the vaccine’s ability to prevent the emergence of new variants since most novel variants come from persistent infections in immunocompromised individuals.
Appendix
Let’s suppose there is a future novel SARS-CoV-2 variant that is as different from current circulating variants as Omicron BA.1 was from the Delta variant. A UK study found that, among individuals with 2 COVID vaccine doses, the onward non-household adjusted secondary attack rate was ~3.7% for Delta as compared to ~7.5% for Omicron. And among the unvaccinated, the non-household adjusted secondary attack rate was ~4.9% for Delta, compared to ~8.8% for Omicron.
Let’s assume the following initial values and parameters:
- Population: 100,000
- Vaccination rate: 69.5% of U.S. population have completed primary series (usually, 2 doses)
- Secondary attack rates:
- Vaccinated: 3.7% for Delta and 7.5% for Omicron
- Unvaccinated: 4.9% for Delta and 8.8% for Omicron
- Initial infected: 10
- Infection rate: adjusted based on secondary attack rates for vaccinated and unvaccinated individuals and the scenarios being considered
- Recovery rate: 0.3
Scenarios:
- Current scenario (no threshold): this represents the scenario in which immunity comparable to that induced by current vaccination is used and there is no set threshold for reduction of viral transmission
- Scenario with 50% threshold: A new 50% threshold target for viral transmission reduction
- Scenario with 70% target: The existing 70% optimal target for viral transmission reduction
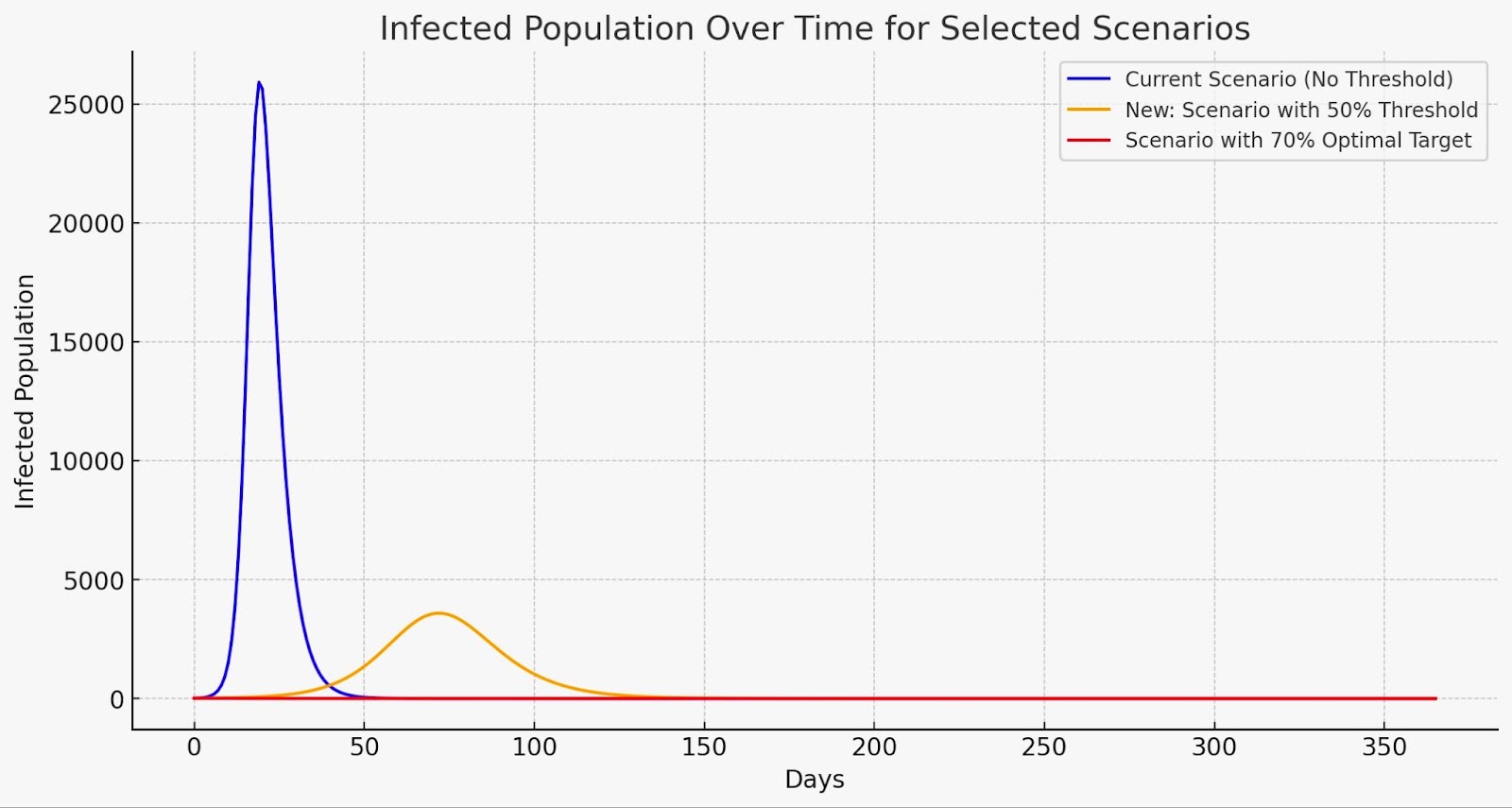
There are many assumptions in this simple SIR model that would of course not hold in reality, but these simulations clearly show there would be a substantial impact of setting a threshold target for viral transmission — in particular, that the setting of higher targets is nonlinear. A new threshold target of 50% provides considerable reduction in infections, while the existing optimal target of 70% would massively reduce the number of infections.